For more information concerning pediatric dentistry, please visit the website for the American Academy of Pediatric Dentistry.
The pediatric dentist has an extra two to three years of specialized training after dental school, and is dedicated to the oral health of children from infancy through the teenage years. The very young, pre-teens, and teenagers all need different approaches in dealing with their behavior, guiding their dental growth and development, and helping them avoid future dental problems. The pediatric dentist is best qualified to meet these needs.
It is very important to maintain the health of the primary teeth. Neglected cavities can and frequently do lead to problems which affect developing permanent teeth. Primary teeth, or baby teeth are important for (1) proper chewing and eating, (2) providing space for the permanent teeth and guiding them into the correct position, and (3) permitting normal development of the jaw bones and muscles. Primary teeth also affect the development of speech and add to an attractive appearance. While the front 4 teeth last until 6-7 years of age, the back teeth (cuspids and molars) aren’t replaced until age 10-13.
 Eruption Of Your Child's Teeth
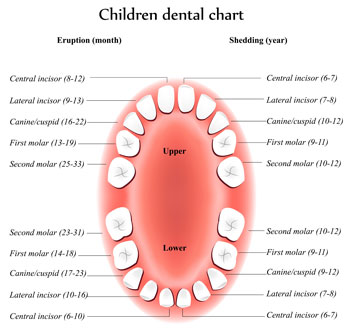
Eruption Of Your Child's TeethChildren’s teeth begin forming before birth. As early as 4 months, the first primary (or baby) teeth to erupt through the gums are the lower central incisors, followed closely by the upper central incisors. Although all 20 primary teeth usually appear by age 3, the pace and order of their eruption varies.
Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors. At the age of 8, you can generally expect the bottom 4 primary teeth (lower central and lateral incisors) and the top 4 primary teeth (upper central and lateral incisors) to be gone and permanent teeth to have taken their place. There is about a one to two year break from ages 8-10 and then the rest of the permanent teeth will start to come in. This process continues until approximately age 21.
Adults have 28 permanent teeth, or up to 32 including the third molars (or wisdom teeth).
 Toothache:
Clean the area of the affected tooth. Rinse the mouth thoroughly with
warm water or use dental floss to dislodge any food that may be
impacted. If the pain still exists, contact your child's dentist. Do
not place aspirin or heat on the gum or on the aching tooth. If the
face is swollen, apply cold compresses and contact your dentist
immediately.
Toothache:
Clean the area of the affected tooth. Rinse the mouth thoroughly with
warm water or use dental floss to dislodge any food that may be
impacted. If the pain still exists, contact your child's dentist. Do
not place aspirin or heat on the gum or on the aching tooth. If the
face is swollen, apply cold compresses and contact your dentist
immediately.
Cut or Bitten Tongue, Lip or Cheek: Apply ice to injured areas to help control swelling. If there is bleeding, apply firm but gentle pressure with a gauze or cloth. If bleeding cannot be controlled by simple pressure, call a doctor or visit the hospital emergency room.
Knocked Out Permanent Tooth: If possible, find the tooth. Handle it by the crown, not by the root. You may rinse the tooth with water only. DO NOT clean with soap, scrub or handle the tooth unnecessarily. Inspect the tooth for fractures. If it is sound, try to reinsert it in the socket. Have the patient hold the tooth in place by biting on a gauze or clean cloth. If you cannot reinsert the tooth, transport the tooth in a cup containing the patient’s saliva or milk, NOT water. If the patient is old enough, the tooth may also be carried in the patient’s mouth (beside the cheek). The patient must see a dentist IMMEDIATELY! Time is a critical factor in saving the tooth.
Knocked Out Baby Tooth: Contact your pediatric dentist. Unlike with a permanent tooth, the baby tooth should not be replanted due to possible damage to the developing permanent tooth. In most cases, no treatment is necessary.
Chipped/Fractured Permanent Tooth: Time is a critical factor, contact your pediatric dentist immediately so as to reduce the chance for infection or the need for extensive dental treatment in the future. Rinse the mouth with water and apply a cold compress to reduce swelling. If you can find the broken tooth piece, bring it with you to the dentist.
Chipped/Fractured Baby Tooth: Contact your pediatric dentist.
Severe Blow to the Head: Call 911 immediately or ake your child to the nearest hospital emergency room.
Possible Broken or Fractured Jaw: Keep the jaw from moving and take your child to the nearest hospital emergency room.
Read more about how to prevent dental emergencies during recreational activities and sports with mouth guards.
 Radiographs (X-Rays) are a vital and necessary part of your child’s
dental diagnostic process. Without them, certain dental conditions can
and will be missed.
Radiographs (X-Rays) are a vital and necessary part of your child’s
dental diagnostic process. Without them, certain dental conditions can
and will be missed.
Radiographs detect much more than cavities. For example, radiographs may be needed to survey erupting teeth, diagnose bone diseases, evaluate the results of an injury, or plan orthodontic treatment. Radiographs allow dentists to diagnose and treat health conditions that cannot be detected during a clinical examination. If dental problems are found and treated early, dental care is more comfortable for your child and more affordable for you.
The American Academy of Pediatric Dentistry recommends radiographs and examinations every six months for children with a high risk of tooth decay. On average, most pediatric dentists request radiographs approximately once a year. Approximately every 3 years, it is a good idea to obtain a complete set of radiographs, either a panoramic and bitewings or periapicals and bitewings.
Pediatric dentists are particularly careful to minimize the exposure of their patients to radiation. With contemporary safeguards, the amount of radiation received in a dental X-ray examination is extremely small. The risk is negligible. In fact, the dental radiographs represent a far smaller risk than an undetected and untreated dental problem. Lead body aprons and shields will protect your child. Today’s equipment filters out unnecessary x-rays and restricts the x-ray beam to the area of interest. High-speed film and proper shielding assure that your child receives a minimal amount of radiation exposure.
 What's The Best Toothpaste For My Child?
What's The Best Toothpaste For My Child?Tooth brushing is one of the most important tasks for good oral health. Many toothpastes, and/or tooth polishes, however, can damage young smiles. They contain harsh abrasives, which can wear away young tooth enamel. When looking for a toothpaste for your child, make sure to pick one that is recommended by the American Dental Association as shown on the box and tube. These toothpastes have undergone testing to insure they are safe to use.
Use only a smear of toothpaste (the size of a grain of rice) to brush the teeth of a child less than 3 years of age. For children 3 to 6 years old, use a "pea-size" amount of toothpaste and perform or assist your child’s toothbrushing. Remember that young children do not have the ability to brush their teeth effectively on their own. Children should spit out and not swallow excess toothpaste after brushing
Parents are often concerned about the nocturnal grinding of teeth (bruxism). Often, the first indication is the noise created by the child grinding on their teeth during sleep. Or, the parent may notice wear (teeth getting shorter) to the dentition. One theory as to the cause involves a psychological component. Stress due to a new environment, divorce, changes at school; etc. can influence a child to grind their teeth. Another theory relates to pressure in the inner ear at night. If there are pressure changes (like in an airplane during take-off and landing, when people are chewing gum, etc. to equalize pressure) the child will grind by moving his jaw to relieve this pressure.
The majority of cases of pediatric bruxism do not require any treatment. If excessive wear of the teeth (attrition) is present, then a mouth guard (night guard) may be indicated. The negatives to a mouth guard are the possibility of choking if the appliance becomes dislodged during sleep and it may interfere with growth of the jaws. The positive is obvious by preventing wear to the primary dentition.
The good news is most children outgrow bruxism. The grinding decreases between the ages 6-9 and children tend to stop grinding between ages 9-12. If you suspect bruxism, discuss this with your pediatrician or pediatric dentist.
 Thumb or finger sucking or pacifiers can be quite soothing to infants and young children. So while we don’t want to completely discourage your child from thumb or pacifier sucking, we also don’t want it to go on for too long, because dental or skeletal deformations may develop as a result. Therefore, Dr. Mujica would like your child’s thumb sucking to stop by the time he or she is three years old. If you’re having trouble convincing your child to stop sucking his thumb, let us know at your child’s next dental checkup. We have some tips.
Thumb or finger sucking or pacifiers can be quite soothing to infants and young children. So while we don’t want to completely discourage your child from thumb or pacifier sucking, we also don’t want it to go on for too long, because dental or skeletal deformations may develop as a result. Therefore, Dr. Mujica would like your child’s thumb sucking to stop by the time he or she is three years old. If you’re having trouble convincing your child to stop sucking his thumb, let us know at your child’s next dental checkup. We have some tips.
The pulp of a tooth is the inner, central core of the tooth. The pulp contains nerves, blood vessels, connective tissue and reparative cells. The purpose of pulp therapy in Pediatric Dentistry is to maintain the vitality of the affected tooth (so the tooth is not lost).
Dental caries (cavities) and traumatic injury are the main reasons for a tooth to require pulp therapy. Pulp therapy is often referred to as a "nerve treatment", "children's root canal", "pulpectomy" or "pulpotomy". The two common forms of pulp therapy in children's teeth are the pulpotomy and pulpectomy.
A pulpotomy removes the diseased pulp tissue within the crown portion of the tooth. Next, an agent is placed to prevent bacterial growth and to calm the remaining nerve tissue. This is followed by a final restoration (usually a stainless steel crown).
A pulpectomy is required when the entire pulp is involved (into the root canal(s) of the tooth). During this treatment, the diseased pulp tissue is completely removed from both the crown and root. The canals are cleansed, disinfected and, in the case of primary teeth, filled with a resorbable material. Then, a final restoration is placed. A permanent tooth would be filled with a non-resorbing material.
 Developing
malocclusions, or bad bites, can be recognized as early as 2-3 years
of age. Often, early steps can be taken to reduce the need for major
orthodontic treatment at a later age.
Developing
malocclusions, or bad bites, can be recognized as early as 2-3 years
of age. Often, early steps can be taken to reduce the need for major
orthodontic treatment at a later age.
Stage I – Early Treatment: This period of treatment encompasses ages 2 to 6 years. At this young age, we are concerned with underdeveloped dental arches, the premature loss of primary teeth, and harmful habits such as finger or thumb sucking. Treatment initiated in this stage of development is often very successful and many times, though not always, can eliminate the need for future orthodontic/orthopedic treatment.
Stage II – Mixed Dentition: This period covers the ages of 6 to 12 years, with the eruption of the permanent incisor (front) teeth and 6 year molars. Treatment concerns deal with jaw malrelationships and dental realignment problems. This is an excellent stage to start treatment, when indicated, as your child’s hard and soft tissues are usually very responsive to orthodontic or orthopedic forces.
Stage III – Adolescent Dentition: This stage deals with the permanent teeth and the development of the final bite relationship.
 Adult Teeth Coming in Behind Baby Teeth
Adult Teeth Coming in Behind Baby TeethThis is a very common occurrence with children, usually the result of a lower, primary (baby) tooth not falling out when the permanent tooth is coming in. In most cases if the child starts wiggling the baby tooth, it will usually fall out on its own within two months. If it doesn't, then contact your pediatric dentist, where they can easily remove the tooth. The permanent tooth should then slide into the proper place.
In most cases, Dr. Mujica repairs a cavity with a tooth-colored filling. Made of composite resin materials, these fillings blend seamlessly with the shading of your child’s natural smile. Moreover, the material is strong, durable and requires less tooth preparation than a metal filling. That means your child spends less time with a dental drill in his or her mouth.
If tooth decay is so severe that a filling will not do, then a dental crown may be the best solution. A crown may also be called for in case of injury that damages a tooth. A crown, which can be made of porcelain, metal or ceramics, completely covers a tooth. Dr. Mujica will prepare the tooth by removing decay and contouring the tooth. Then, the customized crown is cemented into place.
For an infected tooth, root canal therapy may be necessary. Please don’t think that your child will be in pain during a root canal. To the contrary, a root canal is designed to eliminate the pain of an infected tooth. With special tools, Dr. Mujica accesses the tooth’s innermost pulp chamber to remove the infection and replace it with a biocompatible material. The Charlotte pediatric dentist completes the treatment with a protective dental crown.
For more information about restorative dentistry for your children, or to schedule an appointment, call All Kids Pediatric Dentistry in Charlotte, NC, at (980) 263-2330.
 The
American Academy of Pediatric Dentistry (AAPD) recommends that all
pregnant women receive oral healthcare and counseling during
pregnancy. Research has shown evidence that periodontal disease can
increase the risk of preterm birth and low birth weight. Talk to your
doctor or dentist about ways you can prevent periodontal disease
during pregnancy.
The
American Academy of Pediatric Dentistry (AAPD) recommends that all
pregnant women receive oral healthcare and counseling during
pregnancy. Research has shown evidence that periodontal disease can
increase the risk of preterm birth and low birth weight. Talk to your
doctor or dentist about ways you can prevent periodontal disease
during pregnancy.
Additionally, mothers with poor oral health may be at a greater risk of passing the bacteria which causes cavities to their young children. Mother's should follow these simple steps to decrease the risk of spreading cavity-causing bacteria:
The American Academy of Pediatrics (AAP), the American Dental Association (ADA), and the American Academy of Pediatric Dentistry (AAPD) all recommend establishing a "Dental Home" for your child by one year of age. Children who have a dental home are more likely to receive appropriate preventive and routine oral health care.
The Dental Home is intended to provide a place other than the Emergency Room for parents.
You can make the first visit to the dentist enjoyable and positive. If old enough, your child should be informed of the visit and told that the dentist and their staff will explain all procedures and answer any questions. The less to-do concerning the visit, the better.
It is best if you refrain from using words around your child that might cause unnecessary fear, such as needle, pull, drill or hurt. Pediatric dental offices make a practice of using words that convey the same message, but are pleasant and non-frightening to the child.
Teething, the process of baby (primary) teeth coming through the
gums into the mouth, is variable among individual babies. Some babies
get their teeth early and some get them late. In general, the first
baby teeth to appear are usually the lower front (anterior) teeth and
they usually begin erupting between the age of 6-8 months.
See
"Eruption of Your Child’s Teeth" for more details.
 One
serious form of decay among young children is baby bottle tooth decay.
This condition is caused by frequent and long exposures of an infant’s
teeth to liquids that contain sugar. Among these liquids are milk
(including breast milk), formula, fruit juice and other sweetened
drinks.
One
serious form of decay among young children is baby bottle tooth decay.
This condition is caused by frequent and long exposures of an infant’s
teeth to liquids that contain sugar. Among these liquids are milk
(including breast milk), formula, fruit juice and other sweetened
drinks.
Putting a baby to bed for a nap or at night with a bottle other than water can cause serious and rapid tooth decay. Sweet liquid pools around the child’s teeth giving plaque bacteria an opportunity to produce acids that attack tooth enamel. If you must give the baby a bottle as a comforter at bedtime, it should contain only water. If your child won't fall asleep without the bottle and its usual beverage, gradually dilute the bottle's contents with water over a period of two to three weeks.
After each feeding, wipe the baby’s gums and teeth with a damp washcloth or gauze pad to remove plaque. The easiest way to do this is to sit down, place the child’s head in your lap or lay the child on a dressing table or the floor. Whatever position you use, be sure you can see into the child’s mouth easily.
Sippy cups should be used as a training tool from the bottle to a cup and should be discontinued by the first birthday. If your child uses a sippy cup throughout the day, fill the sippy cup with water only (except at mealtimes). By filling the sippy cup with liquids that contain sugar (including milk, fruit juice, sports drinks, etc.) and allowing a child to drink from it throughout the day, it soaks the child’s teeth in cavity causing bacteria.

Children’s dentistry actually begins with you. Even before your child has any teeth, dental care is important. Those beautiful pearly whites are just waiting to erupt through the gums. So, after every feeding, be sure to wipe your baby’s gums with a soft, damp washcloth. This will remove plaque and any formula or breastmilk. If you are bottle-feeding, don’t let your baby fall asleep with a bottle of milk or juice, which both contain sugars that can cause cavities to develop.
Once that first little tooth arrives, it’s time to start brushing. Use a soft baby toothbrush that is moistened with water. There’s no need to use toothpaste yet. As your child grows and more teeth erupt, you can add a minimal amount of fluoride toothpaste.
Try to minimize the amount of toothpaste your child swallows. If your child is too young to spit, then just smear a small amount of toothpaste on the brush. As they learn to spit, you can use a pea-size amount of toothpaste. You’ll need to help your children brush and floss at least until they are seven or eight years old. When they start brushing and flossing on their own, they still might need your help. They should brush their teeth at least two times each day. Be sure to choose a toothpaste that is approved for children by the American Dental Association. Very often, toothpaste for adults contains abrasives that can be damaging to developing teeth. Flossing should happen every night before bed, and may need supervision longer than brushing.
In keeping with the recommendation of the American Academy of Pediatric Dentistry, Dr. Mujica would like to begin seeing your children for regular checkups on or before their first birthdays. Starting this young, your children will become accustomed to seeing the dentist and will begin a lifelong foundation of dental health care.
 Just as the rest of your children’s growing bodies need good nutrition to develop, so do their teeth. A nutritious and well-balanced diet are required for healthy teeth and gums. Ideally, your child’s daily diet should include one or more servings of milk, fruits, vegetable, meat or beans, grains and essential oils. You can review the American Academy of Pediatric Dentistry’s Recommended Food Intake Patterns document here.
Just as the rest of your children’s growing bodies need good nutrition to develop, so do their teeth. A nutritious and well-balanced diet are required for healthy teeth and gums. Ideally, your child’s daily diet should include one or more servings of milk, fruits, vegetable, meat or beans, grains and essential oils. You can review the American Academy of Pediatric Dentistry’s Recommended Food Intake Patterns document here.
For more information about your child’s oral health, or to schedule an appointment, call All Kids Pediatric Dentistry in Charlotte, NC, at (980) 223-3411.
Good oral hygiene removes bacteria and the left over food particles that combine to create cavities. For infants, use a wet gauze or clean washcloth to wipe the plaque from teeth and gums. Avoid putting your child to bed with a bottle filled with anything other than water. See "Baby Bottle Tooth Decay" for more information.
For older children, brush their teeth at least twice a day. Also, watch the number of snacks containing sugar that you give your children.
The American Academy of Pediatric Dentistry recommends visits every six months to the pediatric dentist, beginning at your child’s first birthday. Routine visits will start your child on a lifetime of good dental health.
Your pediatric dentist may also recommend protective sealants or home fluoride treatments for your child. Sealants can be applied to your child’s molars to prevent decay on hard to clean surfaces.
A sealant is a protective coating that is applied to the chewing surfaces (grooves) of the back teeth (premolars and molars), where four out of five cavities in children are found. This sealant acts as a barrier to food, plaque and acid, thus protecting the decay-prone areas of the teeth.

Before Sealant Applied

After Sealant Applied
Fluoride is a natural mineral that attracts other minerals and thereby strengthens tooth enamel. In addition, fluoride inhibits the growth of bacteria that can cause a cavity. Therefore, Dr. Mujica may recommend fluoride treatments. On the other hand, too much fluoride can be harmful to your children’s smiles. With too much fluoride in their diets, children can develop fluorosis, which causes white spots or streaks to develop on their teeth. In severe cases, tooth enamel may turn brown. To prevent fluorosis, make sure your children do not swallow fluoridated toothpaste. Until you know they can spit, either eliminate toothpaste or use a very small amount.
Dental sealants form a solid layer of protection on top of your children’s molars to help them in the battle against tooth decay. Sealants start out as a liquid plastic that we “paint” on the chewing surface of your children’s teeth. Once dried with a curing light, sealants are barrier between the bacteria that cause cavities and your children’s deeply grooved and pitted molars.
 Whether a child is engaging in collision sports such as hockey and football or simply part of a dance class or track team, acrylic mouth guards protect young mouths from soft tissue lacerations, chronic teeth clenching and grinding, tooth avulsion, chips and cracks. The stability and strength conferred by a mouthguard also reduces the chances of jaw fracture and dislocation.
Whether a child is engaging in collision sports such as hockey and football or simply part of a dance class or track team, acrylic mouth guards protect young mouths from soft tissue lacerations, chronic teeth clenching and grinding, tooth avulsion, chips and cracks. The stability and strength conferred by a mouthguard also reduces the chances of jaw fracture and dislocation.
Formed from BPA-acrylic according to oral impressions taken at All Kids Pediatric Dentistry, a sports mouthguard takes an impact so a child’s teeth, gums and jaw don’t have to. The American Dental Association says these mouthguards protect better and are more comfortable than store bought appliances. Your Charlotte children’s dentist can help you decide what device is best for your child and his or her particular activity.
In the safest of athletic activities, accidents happen. An elbow to the mouth knocks out a tooth. A child falls face first off his bike, cutting her bottom lip. Two softball players collide, cracking and chipping front teeth.
Pediatric dental injuries require immediate consultation and treatment with your pediatric dentist in Charlotte, NC. Even when the injured tooth is a baby tooth, act quickly to save it as primary teeth allow for normal eating and speaking and for proper eruption and alignment in the mouth.
Here are practical action items when children suffer dental injury to teeth, gums and jaw:
In the Charlotte area, call Dr. Mujica’s office staff with immediate concerns post sports injury. The right advice and treatment from a dentist who knows the particular needs of children can make the difference between saving and losing good oral function, health and appearance.
The American Academy of Pediatric Dentistry (AAPD) recognizes the benefits of xylitol on the oral health of infants, children, adolescents, and persons with special health care needs.
The use of XYLITOL GUM by mothers (2-3 times per day) starting 3 months after delivery and until the child was 2 years old, has proven to reduce cavities up to 70% by the time the child was 5 years old.
Studies using xylitol as either a sugar substitute or a small dietary addition have demonstrated a dramatic reduction in new tooth decay, along with some reversal of existing dental caries. Xylitol provides additional protection that enhances all existing prevention methods. This xylitol effect is long-lasting and possibly permanent. Low decay rates persist even years after the trials have been completed.
Xylitol is widely distributed throughout nature in small amounts. Some of the best sources are fruits, berries, mushrooms, lettuce, hardwoods, and corn cobs. One cup of raspberries contains less than one gram of xylitol.
Studies suggest xylitol intake that consistently produces positive results ranged from 4-20 grams per day, divided into 3-7 consumption periods. Higher results did not result in greater reduction and may lead to diminishing results. Similarly, consumption frequency of less than 3 times per day showed no effect.
To find gum or other products containing xylitol, try visiting your local health food store or search the Internet to find products containing 100% xylitol.
 Due
to the high sugar content and acids in sports drinks, they have
erosive potential and the ability to dissolve even fluoride-rich
enamel, which can lead to cavities.
Due
to the high sugar content and acids in sports drinks, they have
erosive potential and the ability to dissolve even fluoride-rich
enamel, which can lead to cavities.
To minimize dental problems, children should avoid sports drinks and hydrate with water before, during and after sports. Be sure to talk to your pediatric dentist before using sports drinks.
If sports drinks are consumed:
 You might not be surprised anymore to see people with pierced
tongues, lips or cheeks, but you might be surprised to know just how
dangerous these piercings can be.
You might not be surprised anymore to see people with pierced
tongues, lips or cheeks, but you might be surprised to know just how
dangerous these piercings can be.
There are many risks involved with oral piercings, including chipped or cracked teeth, blood clots, blood poisoning, heart infections, brain abscess, nerve disorders (trigeminal neuralgia), receding gums or scar tissue. Your mouth contains millions of bacteria, and infection is a common complication of oral piercing. Your tongue could swell large enough to close off your airway!
Common symptoms after piercing include pain, swelling, infection, an increased flow of saliva and injuries to gum tissue. Difficult-to-control bleeding or nerve damage can result if a blood vessel or nerve bundle is in the path of the needle.
So follow the advice of the American Dental Association and give your mouth a break – skip the mouth jewelry.
Tobacco in any form can jeopardize your child’s health and cause incurable damage. Teach your child about the dangers of tobacco.
Smokeless tobacco, also called spit, chew or snuff, is often used by teens who believe that it is a safe alternative to smoking cigarettes. This is an unfortunate misconception. Studies show that spit tobacco may be more addictive than smoking cigarettes and may be more difficult to quit. Teens who use it may be interested to know that one can of snuff per day delivers as much nicotine as 60 cigarettes. In as little as three to four months, smokeless tobacco use can cause periodontal disease and produce pre-cancerous lesions called leukoplakias.
If your child is a tobacco user you should watch for the following that could be early signs of oral cancer:
Because the early signs of oral cancer usually are not painful, people often ignore them. If it’s not caught in the early stages, oral cancer can require extensive, sometimes disfiguring, surgery. Even worse, it can kill.
Help your child avoid tobacco in any form. By doing so, they will avoid bringing cancer-causing chemicals in direct contact with their tongue, gums and cheek.